Call Us: (267) 727-3738

Getting to the Crux of a Hip Lux: Diagnosis and Treatment Options

Author: Nina Samuel, VMD, DACVS-SA (Surgeon)
Philadelphia Animal Specialty and Emergency
Hip luxation is the most common joint luxation, and occurs most frequently secondary to vehicular trauma. 75% of luxations occur in a craniodorsal direction, so we will focus on treatment options for this type. More emergent concurrent injuries and trauma should be addressed prior to intervention for an injury to the hip.
Diagnosis
Typical physical examination findings for craniodorsal hip luxation:
If unilateral, patients are generally ambulatory and may be non weight-bearing or weight-bearing (though lame) on the affected limb.
Pain on palpation and range of motion of the affected hip
External rotation, adduction, and apparent shortening of the affected limb
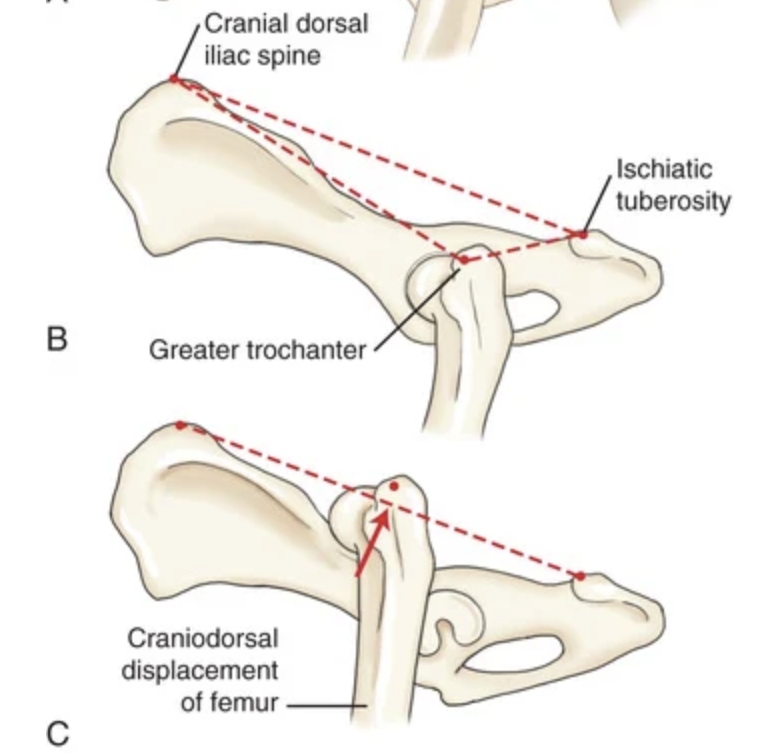
With a normal hip joint, the greater trochanter should be positioned distal to the axis of a line drawn from the craniodorsal border of the iliac spine to the ischial tuberosity, creating a triangle if a finger is placed on each landmark. With a craniodorsal hip luxation, this triangle becomes closer to a straight line.
Pelvis radiographs: Standard two-view orthogonal pelvic radiographs confirm the diagnosis and direction of the hip luxation. Radiographs also allow evaluation of the joint for concurrent fractures and examination of the affected and contralateral hip joints for evidence of hip dysplasia/joint laxity/osteoarthritis, both of which can influence options for intervention.
So you’ve diagnosed a craniodorsal hip luxation! What next?
- Should closed reduction be attempted?
Closed reduction can be attempted as an initial treatment if the hip joint otherwise appears normal (i.e. no fractures and no evidence of hip dysplasia).
Should be attempted within 72 hours of the initial injury as reduction becomes much more difficult with higher reluxation rates due to pathologic changes to the femoral head and acetabulum following this time frame.
Reluxation rates are reported to be upwards of 50% with closed reduction. Though the rate of reluxation is high, attempting closed reduction initially does not affect long-term prognosis with open surgical reduction afterwards.
Resource for a step by step guide on closed reduction: https://www.cliniciansbrief.com/article/closed-hip-reduction
Augmentation of closed reduction with an Ehmer sling may reduce relaxation rates. However, Ehmer slings can also result in severe soft tissue injury. In a recent study (Schlag JAVMA 2019), 50% of dogs had sling-associated soft tissue injuries, with an increased risk for dogs with poorly compliant owners, dogs with soiled/wet bandages, or dogs with a sling placed by an intern rather than a board-certified surgeon or resident.
- When should you recommend open reduction as an initial treatment?
Presence of acetabular or femoral head fractures
Reluxation following radiographically confirmed closed reduction
Concurrent injuries that require immediate function of the hip joint
Chronic luxation
Open reduction and stabilization procedures:
A variety of open reduction techniques exist and decision making in regards to which technique is employed may be dependent on surgeon preference, patient activity level and body weight, direction of luxation, degree of injury to the joint capsule and cartilage, concurrent injuries, and financial constraints
Reluxation rate for open reduction techniques is ~15%
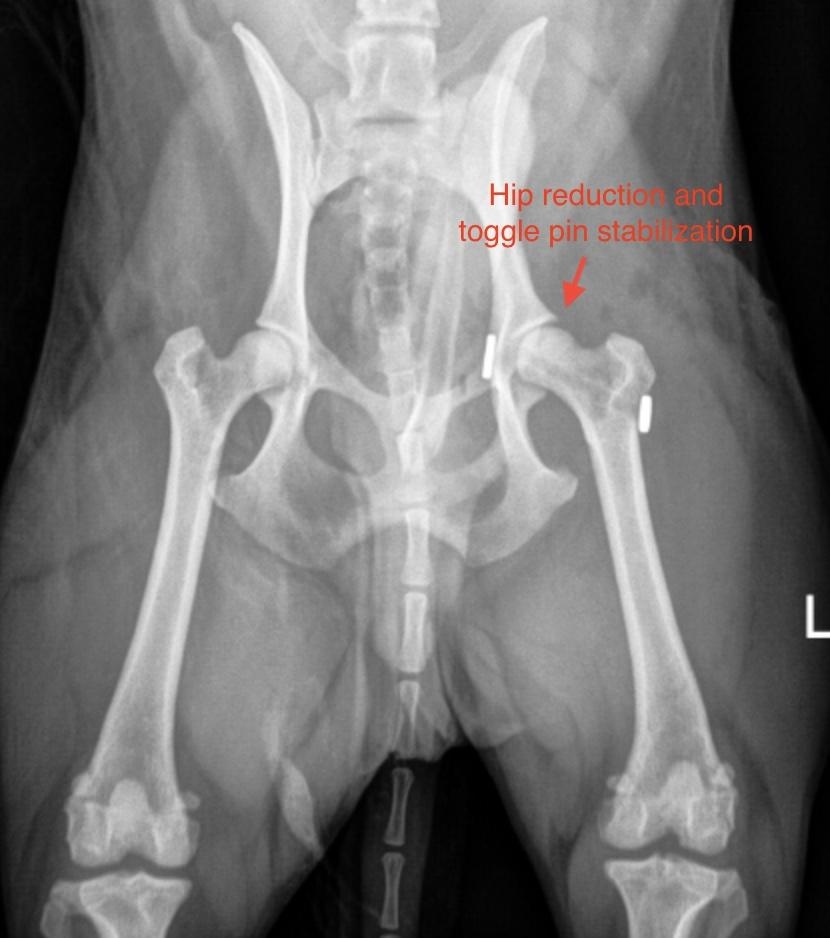
The most common open reduction technique used at PASE is toggle rod stabilization. This uses thick suture material attached to toggle rods/buttons to recreate the ligament of the femoral head and hold the hip in reduction while the peri-articular soft tissues heal. This technique allows early return to weight-bearing.
Salvage procedures:
Salvage procedure techniques may be indicated when there is recurrent femoral head luxation, severe fractures of the acetabulum or femoral head/neck, or if there’s severe osteoarthritis/hip dysplasia affecting the joint
Total hip replacement: In this surgery, the acetabulum and the femoral head and neck are replaced by metal implants to create a synthetic joint. This recreates the hip joint and can allow return to full function.
Femoral head and neck ostectomy: In this surgery, the head and neck of the femur are removed. This surgery removes the pain associated with the hip joint, but results in a gait abnormality as the joint is no longer normal. The function of the joint relies on the muscles surrounding it, and oftentimes physical therapy is indicated and helpful to improve function.
Citations:
Johnston, S. A., & Tobias, K. M. (2017). Veterinary Surgery: Small Animal Expert Consult (2nd ed.). Elsevier - OHCE. https://bookshelf.health.elsevier.com/books/9780323510202
Schlag, A.N., Hayes, G.M., Taylor, A., Kerwin, S.C., Dugat, D.R., Vitt, M.A., Stratton, D.T., & Duffy, D.J. (2019). Analysis of outcomes following treatment of craniodorsal hip luxation with closed reduction and Ehmer sling application in dogs. Journal of the American Veterinary Medical Association, 254 12, 1436-1440.
Phone
Hours
24 Hours A Day / 7 Days A Week
Affiliate Hospital
NorthStar VETS
(609) 259-8300
3 New Jersey Locations
northstarvets.com
© 2026 Philadelphia Animal Specialty & Emergency. All rights Reserved.
Privacy Policy - Sitemap
Powered by