Call Us: (267) 727-3738

Gastric dilatation and volvulus (GDV)

Gastric dilatation and volvulus (GDV) is one of the most life threatening cases that a clinician will encounter. These cases involve gas dilation of the stomach with concurrent rotation along its axis. While it is more commonly reported in dogs, it is possible for cats to develop GDV.
Common Clinical Signs
Non-productive retching
Restlessness
Abdominal distension (not always noticed, especially with significantly deep chested dogs)
Additional clinical signs consistent with shock and cardiovascular collapse
Tachycardia
Weakness
Poor perfusion
Depressed to comatose mentation
Characteristics with Increased Risk of Developing GDV
First degree relative with GDV
Lean body condition
Feeding one large meal a day
Overeating
Speed of eating
Small kibble size
Elevated feeding bowls
Aerophagia
Exercise
Anesthesia
Previous splenectomy (grange 2012)
Inflammatory bowel disease
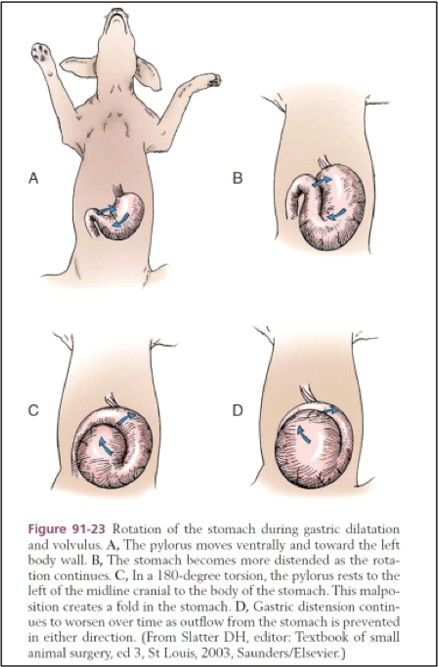
Pathophysiology
Dilatation: Accumulation of gas, often secondary to causes listed above.
Volvulus: Rotation of the stomach along its long axis, often resulting in occlusion of the pylorus and duodenum, impairing venous return and leading to hypovolemic shock.
Diagnostics
Much of the time, a good physical examination (in addition to good history taking) will clue you in that your patient has a GDV. During an examination, you will likely be able to appreciate gastric tympany
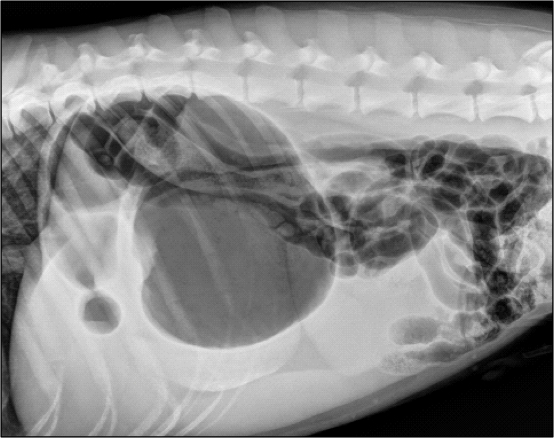
Radiographs: A right lateral radiograph is the most diagnostic. A gas or fluid filled distended stomach with a displaced pylorus – the “double bubble” – as seen below (Photo courtesy of Dr. Adam Yoskowitz VMD DACVR). Consideration for thoracic radiographs should be made based on history, signalment, concern for comorbidities such as aspiration pneumonia and neoplasia.
NB: Prior to taking abdominal radiographs, initial stabilization should be started, see below
Bloodwork: PCV/TS, Venous blood gas, electrolytes, blood glucose, lactate
Predictive value of plasma lactate in GDV?
Lactate <4 mmol/L and/or a >40% reduction in plasma lactate after fluid resuscitation are associated with increased survival and few complications
Lactate >6 mmol/L may be associated with gastric wall necrosis
Initial Management
Intravenous fluid therapy
Goal: rapidly restore circulating blood volume and improve perfusion
Isotonic crystalloids 20-30 ml/kg over 15-30 minutes, based on patient’s response and ongoing losses
Can consider hypertonic saline to reduce the total volume needed to achieve resuscitation endpoints
Analgesia:
Full mu-agonist opioid (hydromorphone, methadone, fentanyl, etc.)
Lidocaine: indicated for patients in ventricular tachycardia and provides analgesia. Lidocaine may reduce risk of cardiac arrythmias and acute kidney injury with possible reduction in hospitalization stay
Decompression of the stomach: Gastric decompression: trocharization (catheterization), orogastric tube
Gastric decompression: No sedation needed
Tools needed: large bore catheter (14-18 gauge), antiseptic solution, sterile gloves, +/- syringe
Positioning: the patient is often in sternal recumbency and while the right side caudal to the ribs is generally the most tympanic, significant gastric tympanic can be appreciated on the left side – if available, an ultrasound probe can help to guide your location by allowing for splenic evaluation.
Prepare the site: After you have located the most tympanic area, clip the fur and clean the skin with antiseptic.
Catheter insertion: holding the catheter perpendicular to the skin, use firm pressure to advance the catheter and stylet through the abdominal wall and into the stomach. Once you hear a rush of gas, remove the stylet and allow the catheter to facilitate gas removal. Once the abdomen returns to normal size, the catheter should be removed.
Risks: inadvertent puncture of other organs
Orogastric tube: Requires sedation
Tools needed: orogastric tube (based on dog’s size), water soluble lubricate, syringe (for aspiration), tape or tube holder, gloves, stethoscope
Positioning: Patient will be in sternal recumbency or standing.
Measurement: Measure the tube from the tip of the nose to the last rib – this will indicate how far to insert the tube.
Prep the tube: Lubricate the tube with water based solution to allow for smooth insertion.
Insertion of the tube: Open the dog’s mouth and gently hold it open. - Introduce the tube into the mouth, directing it along the midline of the tongue and into the oropharynx. - Encourage the dog to swallow by gently stroking the throat or offering a small amount of water if safe to do so.
Advancement of the tube: Continue to advance the tube carefully and steadily until you reach the pre-measured mark. Ensure the tube does not encounter resistance. If resistance occurs, retract the tube slightly and readjust the angle.
Confirm Positioning: Use a syringe to aspirate gastric contents. If the tube is correctly placed in the stomach, you should obtain a small amount of gastric fluid. - Alternatively, place the stethoscope over the dog’s stomach and inject a small amount of air (10-20 mL) through the tube. You should hear a distinct air inflow sound if it’s correctly positioned.
Securing the tube: once confirmed, secure the tube to the dog’s muzzle or a tube holder to prevent displacement. If patient shows evidence of distress or complication, the tube should be removed.
Tube removal: gently remove the tube carefully withdrawing it from the stomach and esophagus.
Risks: aspiration pneumonia, esophageal trauma, gastric perforation
Oxygen therapy if needed
Don’t forget to hook your patient up to monitoring: ECG, blood pressure, pulse oximetry, etc in addition to vitals – serial evaluation of patients allow for appropriate and quick adjustments in therapy for these dynamic cases
Surgical Management vs. Medical Management
Pursuit of medical management portends a higher risk of recurrence, 50-80% which is why GDV is considered a surgical emergency. Immediate laparotomy is essential to untwist the stomach and evaluate for necrosis.
What can you do to give your GDV patient their best chance?
Quick identification of the GDV and rapid intervention! In general, mortality rates are between 10-43 and there is an increased survival associated with rapid intervention. Other contributing factors of increased servival include absence of gastric necrosis, reduction in lactate with treatment, and a serum myoglobin < 168 ng/mL.
Additional References
Beck J, Staatz A, Pelsue D, et al. Risk factors associated with short-term outcome and development of perioperative complications in dogs undergoing surgery because of gastric dilatation-volvulus: 166 cases (1992–2003). J Am Vet Med Assoc 2006;229:1934–1939.
Brourman J, Schertel E, Allen D, et al. Factors associated with perioperative mortality in dogs with surgically managed gastric dilatation-volvulus: 137 cases (1988–1993). J Am Vet Med Assoc 1996;208:1855–1858.
Bruchim Y, Itay S, Shira BH, et al. Evaluation of lidocaine treatment on frequency of cardiac arrhythmias, acute kidney injury, and hospitalization time in dogs with gastric dilatation volvulus. J Vet Emerg Crit Care (San Antonio). 2012;22(4):419-427.
Drobatz, K. J., Hopper, K., Rozanski, E. A., & Silverstein, D. C. (Eds.).(2018). Textbook of small animal emergency medicine. John Wiley & Sons. (pp. 520-523)
Gazzola KM, Nelson LL. The relationship between gastrointestinal motility and gastric dilatation-volvulus in dogs. Top Companion Anim Med. 2014;29(3):64-66.
Grange AM, Clough W, Casale SA. Evaluation of splenectomy as a risk factor for gastric dilatation-volvulus. J Am Vet Med Assoc. 2012;241(4):461-466.
Green T, Tonozzi C, Kirby R, Rudloff E. Evaluation of initial plasma lactate as a predictor of gastric necrosis and initial and subsequent plasma lactate values as a predictor of survival in dogs with gastric dilatation- volvulus: 84 dogs (2003–2007). J Vet Emerg Crit Care 2011;21:36–44.
Phone
Hours
24 Hours A Day / 7 Days A Week
Affiliate Hospital
NorthStar VETS
(609) 259-8300
3 New Jersey Locations
northstarvets.com
© 2026 Philadelphia Animal Specialty & Emergency. All rights Reserved.
Privacy Policy - Sitemap
Powered by