Call Us: (267) 727-3738

Recognizing Proteinuria

Recognizing Proteinuria
Proteinuria is a clinically meaningful marker of disease in dogs and cats, yet its interpretation can be tricky.
Protein detected in urine does not automatically equal kidney disease. Proteinuria is broadly divided into “non-renal”, “renal”, and “post-renal causes”, and identifying the category is essential before treatment decisions are made. Non-renal proteinuria occurs when abnormal proteins circulate in blood and overwhelm normal tubular resorption (examples include hemoglobin, myoglobin, and light chains) or can also originate from genital causes. Renal proteinuria can be functional or pathologic in origin. Functional proteinuria is transient and can be caused by etiologies such as fever, seizures, heavy exercise, venous congestion, amongst others. Pathologic proteinuria is persistent, reflects intrinsic kidney injury/disease, and can be glomerular, tubular, or interstitial in origin. Finally, post-renal proteinuria originates from inflammation or hemorrhage in the urinary or genital tract.
Urine Dipstick
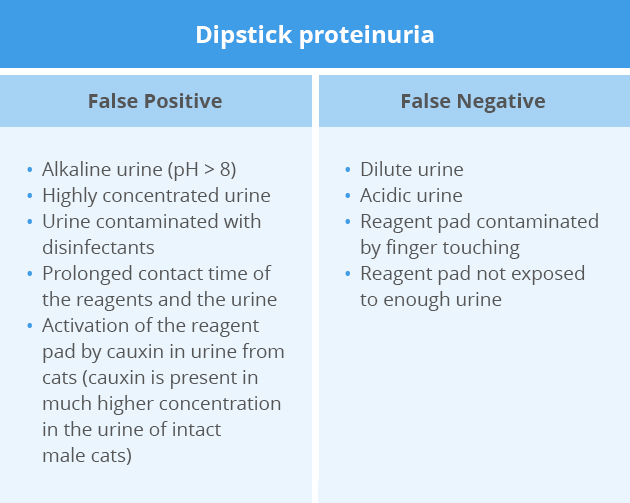
The urine dipstick is the first test performed, which might give information about the presence of proteinuria in a patient. Albumin in the urine readily binds to the indicator dye on the dipstick, resulting in a color reaction. However, a similar result could be seen with other types of protein when present in high enough concentrations in the urine. Therefore a positive color on the reagent pad is not always from albuminuria. Additionally, several factors may result in false positive or false negative results.
The urine concentration is often used in an attempt to help us determine whether a positive urine protein dipstick might or might not be significant. A study (Pérez-Accino, J Small Anim Pract 2020) evaluating the utility of combined urine dipstick analysis and specific gravity (USG) measurement to determine feline proteinuria looked at 121 urine samples and found the dipstick to be inaccurate for detecting proteinuria and grouping the samples by USG did not increase dipstick agreement with the urine protein-creatinine ratio (UPCR). Trace proteinuria (0.1-0.3mg/dL) had a sensitivity of 81% and a specificity of 31% to detect proteinuria. The authors of this study concluded that clinicians should not rely on this test and other quantitative methods such as UPCR should always be performed to detect proteinuria in cats. In dogs, a negative urine dipstick test result (0+) irrespectively of their USG, thereby possibly eliminating the need for determination of the UPCR when a 0+ result is obtained (Zatelli, Am J Vet Res, 2010)
Another study (Fidalgo, Animals 2022) also found that the correlation between UPCR and combined results from dipstick tests and USG is low and inconsistent. Additionally, they demonstrated that proteinuric CKD cats have a worse outcome at both 6 months (odds ratio (OR) 4.04) and 12 months (OR 4.36), and this finding was more pronounced for severely proteinuric cases in which the OR for death was 4.36 and 6.0 at 6 and 12 months, respectively. This not only reinforces the negative prognostic value of proteinuria, but also the importance of measuring UPCR in these patients regardless of the dipstick results obtained and their USG.
Urine protein:creatinine ratio (UPCR)
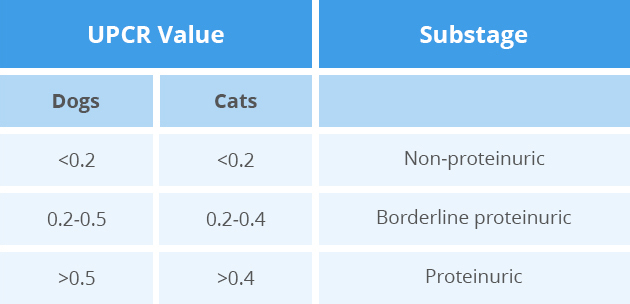
The UPCR allows for the evaluation of the magnitude of proteinuria in a patient. It should be performed as part of further evaluation of dipstick proteinuria as well as in all patients with kidney disease to help determine their substage of proteinuria, help guide therapy, and assess response to therapy.
Monitoring proteinuric patients can be challenging given the day-to-day variation in their UPCR, making it difficult to know what changes are clinically significant. Additionally, UPCR results are higher when measured in urine samples collected at the hospital as opposed to urine samples collected at home, which could have the potential to affect clinical interpretation (Duffy, J Vet Intern Med, 2015). Measuring the UPCR in a pooled sample containing equal volumes of different urine specimens from a given patient is reliable and a cost-effective alternative to assessing multiple UPCR on several specimens from the same patient (Shropshire, J Vet Intern Med, 2018). We recommend that owners collect a urine sample at home on three consecutive days. Once dropped off at the clinic, we obtain 1 mL of urine from each day’s sample and combine them into a single container (total volume = 3mL) for submission.
Implications of proteinuria
Proteinuria is both a biomarker and mediator of renal injury, contributing to ongoing nephron loss and increased risk of CKD progression, uremic decompensation, and mortality. Early identification allows for appropriate diagnostic investigation and timely initiation of therapy aimed at slowing progression.
References
Duffy ME, Specht A, Hill RC. Comparison between urine protein:creatinine ratios of samples obtained from dogs in home and hospital settings. J Vet Intern Med 2015;8:1029-1035. DOI
Fidalgo MA, Leal RO, Duarte-Correia JH. Urinary protein/creatinine ratio in feline medicine: reasons to perform it and its role in clinical practice - a retrospective study. Animals (Basel) 2022;12:1574. DOI
Pérez-Accino J, Bernabe LF, Manzanilla EG, Puig J. The utility of combined urine dipstick analysis and specific gravity measurement to determine feline proteinuria. J Small Anim Pract 2020;61:541-546. DOI
Shropshire S, Quimby J, Cerda R. Comparison of single, averaged, and pooled urine protein:creatinine ratios in proteinuric dogs undergoing medical treatment. J Vet Intern Med 2018;32:288-294. DOI
Zatelli A, Paltrineieri S, Nizi F, et al. Evaluation of a urine dipstick test for confirmation or exclusion of proteinuria in dogs. Am J Vet Res 2010;71:235-240. DOI
Phone
Hours
24 Hours A Day / 7 Days A Week
Affiliate Hospital
NorthStar VETS
(609) 259-8300
3 New Jersey Locations
northstarvets.com
© 2026 Philadelphia Animal Specialty & Emergency. All rights Reserved.
Privacy Policy - Sitemap
Powered by